The Result
Omega-3 is probably one of the most taken supplements in the health-aware community.
But do we really know the goal?
A lot of people take fish oil. Some eat salmon. Some use algae oil. Some avoid seed oils. But because Omega-3 Index is relatively expensive to test, not many people actually know their level.
And we should:
Modelling suggests the gap between a low and high Omega-3 Index may be worth around 4–5 years in predicted life expectancy — comparable in size to the smoking effect in the same model.
It's a serious longevity biomarker.
In the first cohort at Revi Longevity — many of whom already supplement — not many met the grade:
Omega-3 Index ranged from 5.0% to 10.4%
~70% were below the cardiovascular protective threshold of 8% (Harris & von Schacky, 2004)
~90% were below the Revi Optimal band
The great thing is that the index is easy to move — and good levels compound over time.
This is why Revi tests it.
If you're going to take something for years, you should know whether it is working.
The biology
The goal is to maintain the right balance of omega-3s and omega-6s.
They become part of the membranes that surround our cells.
And as we can't efficiently make them ourselves, our diet is a huge contributor:
Omega-3s — found in oily fish, algae, flax/chia/walnuts (less useful).
Omega-6s — found in seed/vegetable oils (sunflower, corn, soybean), processed food, restaurants & takeaways.
The balance, or ratio of these, influences the body's inflammatory position.
The problem in the UK is that many diets lean significantly towards Omega-6s, with very little oily fish intake.
Our average Omega-3 Index is ~4–5%, compared to Japan's average of ~8–10% (Stark et al., 2016), where higher marine omega-3 levels are associated with significantly less atherosclerosis (Sekikawa et al., 2008)
And it's not just for the heart:
Omegas are structural components of cell membranes throughout the body — the heart, the brain, the pancreas, the joints and the skin at the same time.
Longevity — where we want to be
We spoke at the start on statistics — 4–5 years more life in people in the top 20% — a difference comparable in magnitude to that between smokers and non-smokers in the same dataset (McBurney et al., 2021).
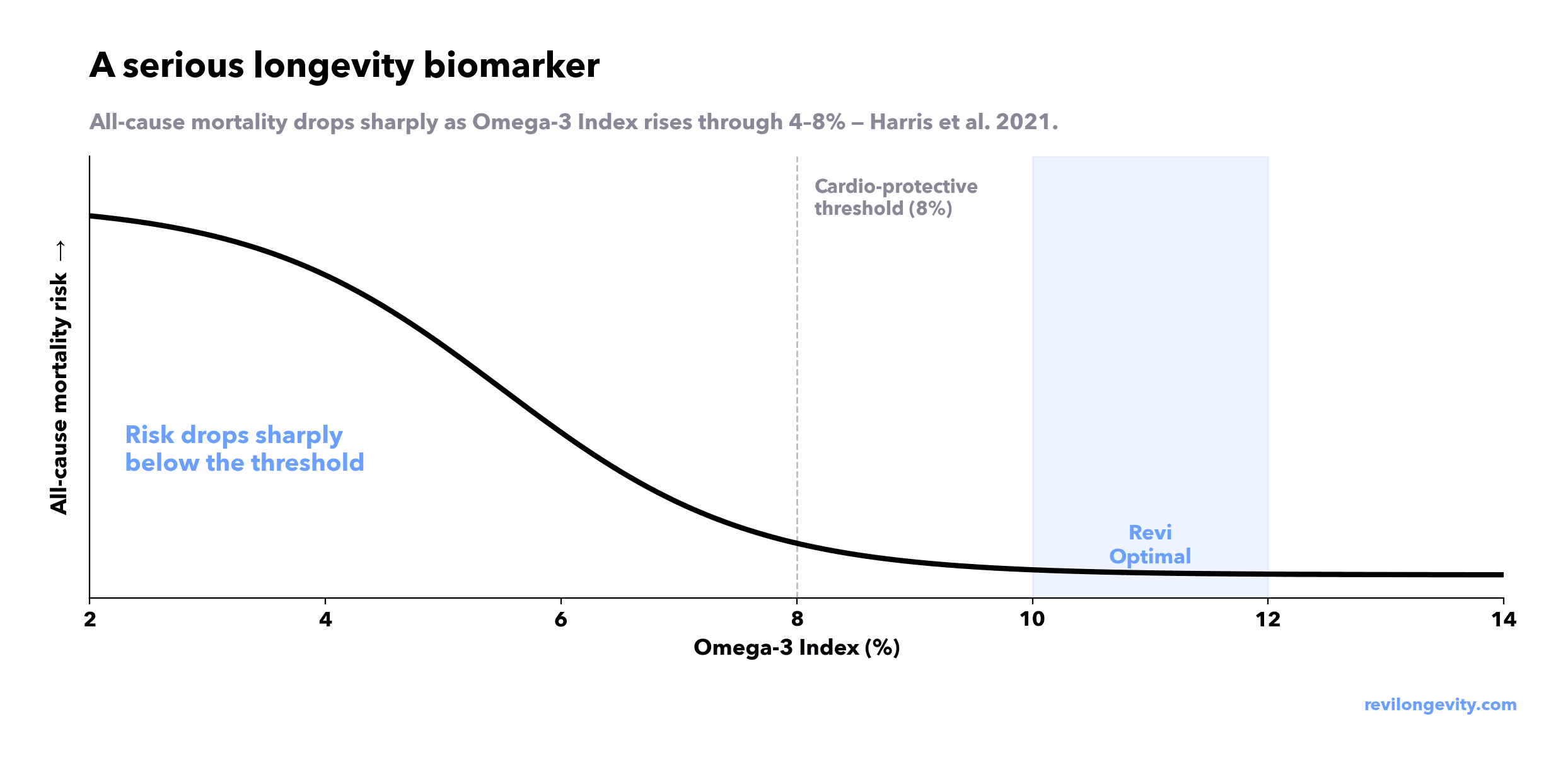
The benefits of higher Omega-3 levels increase linearly until you reach around 8–12% (Harris & von Schacky, 2004; Harris et al., 2021).
More isn't always better — the curve plateaus because the cell membrane fills up, so the benefits of going higher are marginal.
Revi's model uses a tighter 10–12% optimal band for the Omega-3 Index — the upper portion of the validated protective range. Our goal is to optimise, not just avoid risk.
Simple science
Our cell membranes are built up from the fats we eat — both Omega-3s & 6s
When cells are injured or stressed, they pull fat from the membrane to use for signalling
The ratio of fats stored in your membrane (which reflects your diet over months) indicates which is more likely to be used:
Too much 6s and not enough 3s:
Cause blood vessels to widen, swell, and sensitise nerves — more pain. Side bar: Ibuprofen / aspirin block the enzyme which causes this (FitzGerald & Patrono, 2001).
Clumps platelets in blood together — more clotting
Recruits white blood cells — tightens airways
Stronger inflammatory signals — good for an immune response, less useful if elevated over time.
Enough 3s and not too much 6s:
As above but less strong signals
Help the body resolve inflammation — the switch off, clean-up, repair response (Serhan, 2014).
It's not that Omega-6s are bad — the problem is the ratio.
We might have all heard the term 'inflammaging' (Franceschi et al., 2000) — this is it. By having a better ratio, you slow background damage in every tissue at the same time.
The benefits of optimising the Omega-3 index & associated ratios
Better heart health — the lower the Omega-3 Index, the higher the mortality risk (Harris et al., 2021).
Better index →
Less inflammation in arteries → slower plaque → less risk
Less triglycerides in blood → reduced atherogenic load → less risk
Heart membranes more stable → steadier heart rhythm → less risk
Reduced inflammation — omega-3s turn off inflammation; when low, we can't do this
Better fuel handling — omega ratios impact how well insulin works on our cells.
Better index → more fluid membrane and lower inflammatory tone → better sugar handling
Recovery that feels easier — we are able to resolve inflammation faster and properly.
Better skin + joints — lower the inflammatory tone and the tissue settles and recovers faster.
Better mood — omega-3 supplementation has shown benefit for major depression in meta-analysis (Mocking et al., 2016)
Better cognition — DHA supplementation has shown improvements in age-related cognitive decline (Yurko-Mauro et al., 2010).
DHA is the most abundant omega-3 in brain → better DHA → better signalling.
Understanding the Revi biomarkers
These are "optimise in advance" markers, not "you have symptoms" markers. The benefits from maintaining healthy levels compound over time and we avoid poor ratios creeping up on us in 10–20 years.
Marker | What it captures | Target |
|---|---|---|
Omega-3 Index | EPA+DHA as % of red blood cell membrane — the 3-month status anchor. | Higher better up to optimal |
EPA | Anti-inflammatory raw material. | Higher better up to optimal |
AA (Arachidonic Acid) | The main omega-6 in the membrane. Pro-inflammatory raw material. | Not too high, not too low |
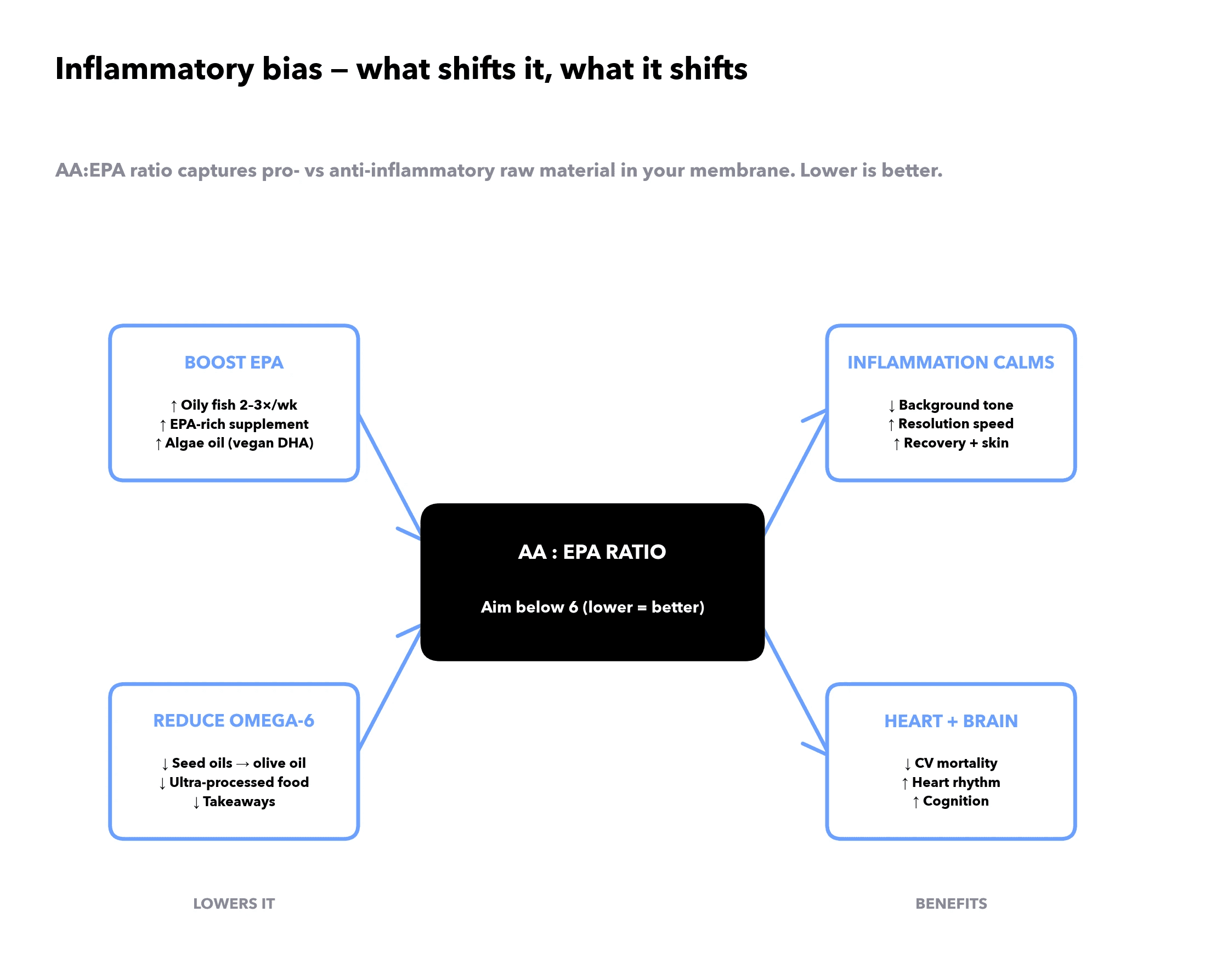
AA:EPA Ratio | Ratio of pro vs anti-inflammatory. | Lower better |
Omega-6/Omega-3 Ratio | The same ratio at the whole-family level. | Lower better |
What levers optimise Omega-3
Red blood cells turn over every ~120 days — so changes in your intake and diet can materially change your markers in a matter of months.
The best approach is to measure, then dose to the right amount for your goals.
Action | Dose | Tier | Effect size |
|---|---|---|---|
EPA/DHA supplement (triglyceride form) | Typically 1–2g combined EPA+DHA/day, with food | A | High — raises Omega-3 Index |
Oily fish 2–3×/week | Salmon, mackerel, sardines, herring, anchovies (not tuna) | A | Med–High — raises Index |
Reduce seed oils / processed food | Swap to olive oil; cut ultra-processed food | B | Med — improves the ratio, modest on absolute Index |
Algae oil (DHA-rich) | 600–1000mg DHA/day | B | Med — vegan route, slightly less efficient per gram |
Krill oil (phospholipid-bound) | 1–2g/day | B | Med — possibly better absorbed, costlier per gram |
ALA sources (flax, chia, walnuts) | 1–2 tbsp ground flaxseed/day | C | Low — ALA→EPA conversion ~5–8% in humans (Burdge & Wootton, 2002) |
Evidence tier:
A = multiple RCTs / meta-analyses
B = strong observational + supporting RCT
C = emerging / mechanistic
For most healthy adults, omega-3 optimisation is a nutrition/supplement lever.
But high-dose omega-3 is not automatically harmless. Anyone with atrial fibrillation, cardiovascular disease, blood-thinning medication, bleeding risk, or planned surgery should discuss higher-dose supplementation with a clinician first (Bhatt et al., 2019).
The Revi Read
A sample of records from our first cohort — most of which were already supplementing.
My Omega-3 sits at 10.37% — inside the Revi optimal band, but it took months of consistent supplementation to get there. See my case study ->
Green = Revi Optimal, Amber = Inside Reference Range, Red = Outside Reference Range.

What's interesting:
Omega-3 Index: ~70% of the cohort were below the cardio-protective threshold (8%).
Omega-6/3: can look fine in isolation; the AA:EPA ratio is the clear inflammatory signal.
AA:EPA: the widest spread in the panel — 6.6 to 42.6, more than a six-fold difference.
What we recommended:
Most could benefit from improving the AA:EPA ratio and boosting Omega-3s as a whole.
A supplement containing high DHA and EPA — noting ensuring the active dose of EPA & DHA is high enough, not just the total oil.
REV000005, REV000006, REV000007 recommended to significantly cut down on seed oils and processed foods.
Re-test the numbers in 3–4 months.
Reading it in context
At Revi we don't just read the fatty acid panel — we consider this in context with your other clustered markers.
Then we prioritise your top actions across the panel.
Related marker | Why it matters here |
|---|---|
hs-CRP | Helps show whether there is broader inflammatory load. |
ApoB | Shows the number of atherogenic particles — key for cardiovascular risk context. |
HDL Cholesterol | HDL has anti-inflammatory and reverse-cholesterol-transport functions. |
The principles
It's "UK longevity bloodwork," not a disease test: we don't wait until a marker is bad — we pursue longevity optimal.
It's only visible because the panel is deep. The fatty-acid axis is six of Revi's 95+ markers. These markers are typically excluded on normal panels due to the price.
Test, don't guess:
Sometimes you measure and find something you didn't know about — we give you the action.
Sometimes you measure and find something working great — we give you the confidence to continue.
References
Bhatt, D.L., Steg, P.G., Miller, M., et al. (2019). Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia (REDUCE-IT). New England Journal of Medicine, 380(1), 11–22.
Burdge, G.C. & Wootton, S.A. (2002). Conversion of alpha-linolenic acid to eicosapentaenoic, docosapentaenoic and docosahexaenoic acids in young women. British Journal of Nutrition, 88(4), 411–420.
FitzGerald, G.A. & Patrono, C. (2001). The Coxibs, selective inhibitors of cyclooxygenase-2. New England Journal of Medicine, 345(6), 433–442.
Franceschi, C., Bonafè, M., Valensin, S., et al. (2000). Inflamm-aging: an evolutionary perspective on immunosenescence. Annals of the New York Academy of Sciences, 908, 244–254.
Harris, W.S. & von Schacky, C. (2004). The Omega-3 Index: a new risk factor for death from coronary heart disease? Preventive Medicine, 39(1), 212–220.
Harris, W.S., Tintle, N.L., Imamura, F., et al. (2021). Blood n-3 fatty acid levels and total and cause-specific mortality from 17 prospective studies. Nature Communications, 12, 2329.
McBurney, M.I., Tintle, N.L., Vasan, R.S., Sala-Vila, A. & Harris, W.S. (2021). Using an erythrocyte fatty acid fingerprint to predict risk of all-cause mortality: the Framingham Offspring Cohort. American Journal of Clinical Nutrition, 114(4), 1447–1454.
Mocking, R.J.T., Harmsen, I., Assies, J., et al. (2016). Meta-analysis and meta-regression of omega-3 polyunsaturated fatty acid supplementation for major depressive disorder. Translational Psychiatry, 6, e756.
Sekikawa, A., Curb, J.D., Ueshima, H., et al. (2008). Marine-derived n-3 fatty acids and atherosclerosis in Japanese, Japanese-American, and white men. Journal of the American College of Cardiology, 52(6), 417–424.
Serhan, C.N. (2014). Pro-resolving lipid mediators are leads for resolution physiology. Nature, 510(7503), 92–101.
Stark, K.D., Van Elswyk, M.E., Higgins, M.R., Weatherford, C.A. & Salem, N. Jr. (2016). Global survey of the omega-3 fatty acids, docosahexaenoic acid and eicosapentaenoic acid in the blood stream of healthy adults. Progress in Lipid Research, 63, 132–152.
Yurko-Mauro, K., McCarthy, D., Rom, D., et al. (2010). Beneficial effects of docosahexaenoic acid on cognition in age-related cognitive decline. Alzheimer's & Dementia, 6(6), 456–464.
Cris Hesketh
Founder, Revi Longevity
revilongevity.com





