The Result:
This one annoyed me. My HbA1c was 40.77 mmol/mol — not diabetes, not technically pre-diabetes — but only 1.23 mmol/mol below the threshold.
How can I train regularly, eat relatively well, and be here?
Across the people I've tested so far, HbA1c ranged from 29.7 to 55.0 mmol/mol — a near two-fold spread:
~30% were optimal (<35)
~55% were in the typical reference range but higher than optimal (35-42)
~15% were in diabetic / pre-diabetic territory.
Only 15% would have been flagged on a standard test - That's the entire problem.
Revi uses optimisation gaps: not yet clinically bad, but closer to the line than we would want.
The biology:
HbA1c: Your 3-month average glucose exposure.
When glucose control is off, it can sometimes show up as energy crashes, hunger after meals, brain fog, slower recovery, or increasing waist/body fat — but symptoms are unreliable, which is why testing matters.
It’s heavily influenced by lifestyle — meals, snacks, alcohol, sleep, stress, movement and training over time.
It’s usually treated as “the diabetes marker”, but long-term glucose exposure also matters for metabolic health, cardiovascular risk, blood vessel health and cognitive ageing.
For scale, 5 million people in the UK live with diabetes — and ~1 million of them don't know it. Add the ~6 million in pre-diabetes and we're at 1 in 5 of the population at risk

Why it matters:
Every 1 mmol/mol increase associates with a measurable increase in all-cause mortality
More glucose exposure = more cardiovascular events, more dementia - continuously increasing as the result increases.
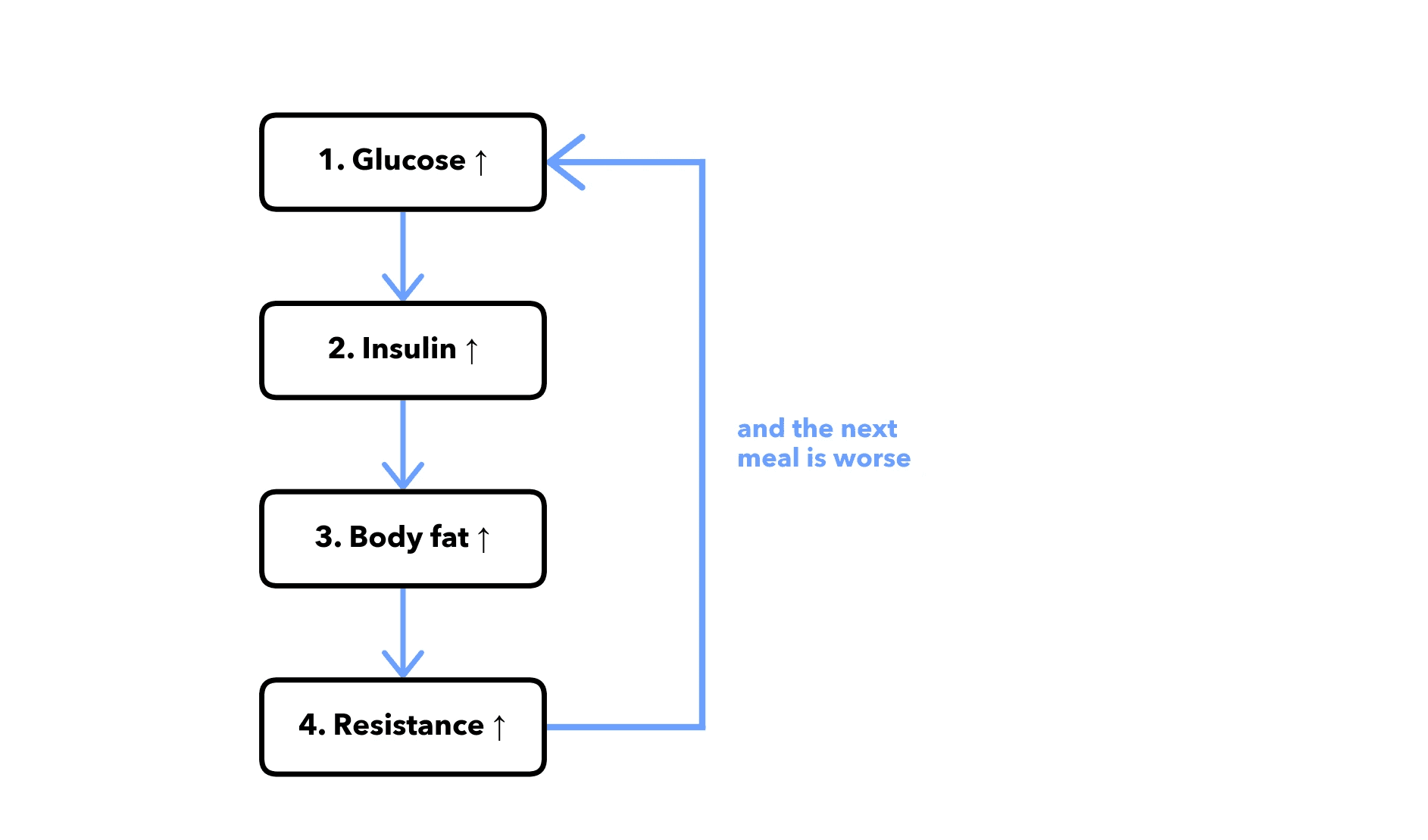
The HbA1c loop:
It’s not just the sugar - it’s what happens after that’s the problem - the longer, and higher it is, the harder it becomes to manage the sugar in the first place.
High glucose → more insulin → more resistance → more body fat → more resistance → higher glucose.
And it's not just glucose. Chronic high insulin keeps the body in 'grow mode’:
We store more fat in belly & around the liver
Cells divide so we can grow (mTOR goes up) but autophagy reduces (the cleanup we require for longevity and cellular repair)
The Levers
The overarching goal:
Keep HbA1c in the optimal zone
Maintain insulin sensitivity for as long as possible
Manage the amount of time blood glucose & insulin are high in the bloodstream.
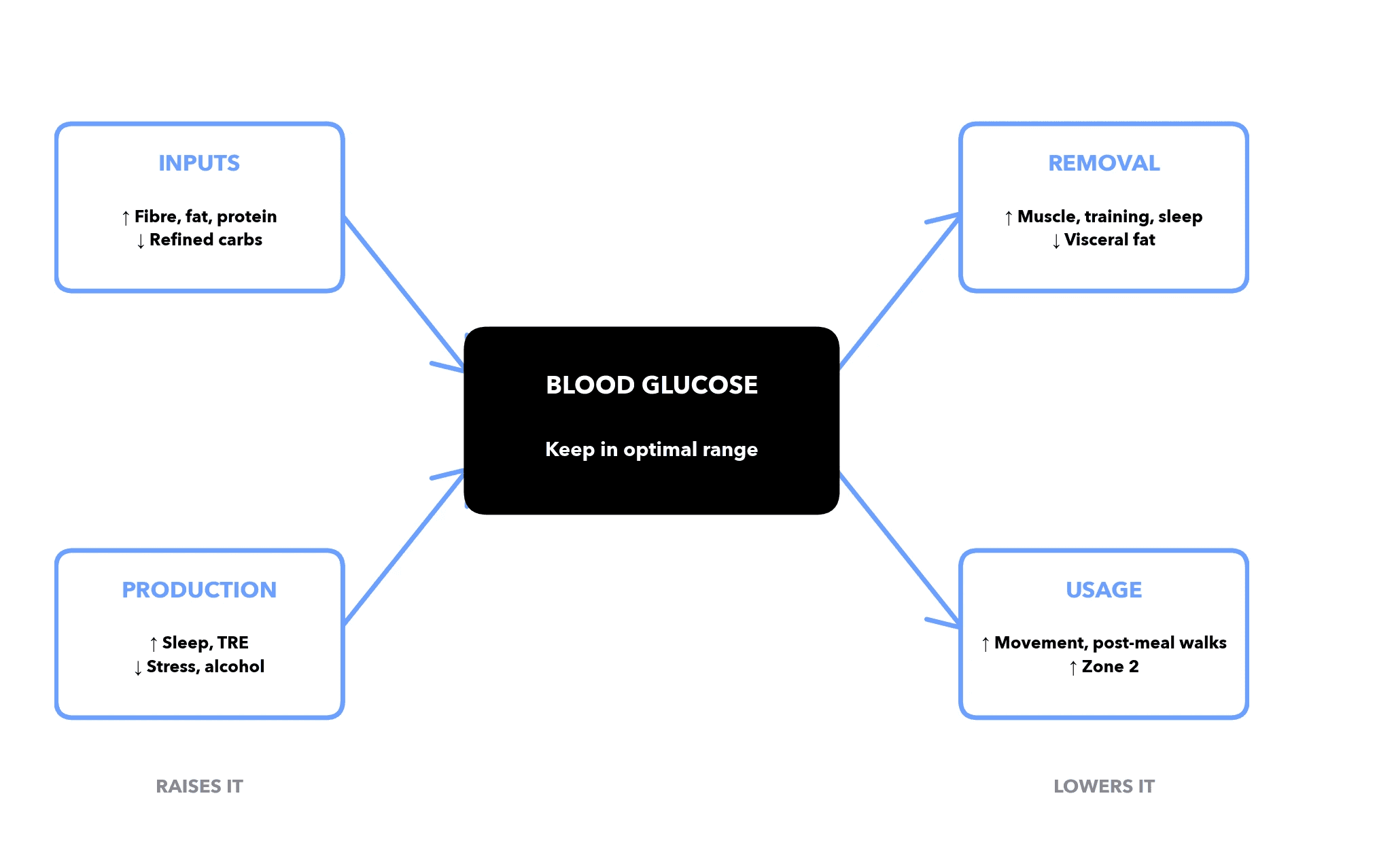
The Four Glucose Levers
Lever | What it is | Mechanism |
|---|---|---|
Inputs | How much, and how quickly it hits us | Glucose enters the bloodstream from food. How fast depends on what's in the meal alongside the carbs. |
Production | How much we make ourselves | The liver produces glucose between meals — but overproduces when stressed and sleep-deprived. |
Removal | How fast we get it out of the blood into cells | Insulin moves glucose from the blood into cells, muscles and the liver — doesn't work as well when insulin-resistant. |
Usage | How much we actually use | Burning the glucose our cells and muscles absorbed. |
Keeping glucose in the optimal range
We need to manage our nutrition, stress, sleep, body composition, and movement.
Which levers matter most
At Revi, we rank interventions by three things: evidence, breadth across the four levers, and effect size. The best ones pull on more than one.
Lever | Action | Ev. | Effect | Inputs | Production | Removal | Usage |
|---|---|---|---|---|---|---|---|
Weight loss (5–10%) | Caloric deficit; preserve muscle | A | High | ✓ | ✓ | ✓ | |
Resistance training | 2–4 sessions/week, full-body, progressive | A | High | ✓ | ✓ | ||
Zone 2 cardio | 150–300 min/week, conversational pace | A | Med | ✓ | ✓ | ||
Time-restricted eating | 8–10h window, earlier is better | B | Med | ✓ | ✓ | ||
Fibre to 30–40g/day | Whole foods, psyllium if needed | A | Med | ✓ | |||
Reduce processed carbs | Cut sugary drinks, white bread, pastries | B | Med | ✓ | |||
Sleep ≥7h/night | Consistent timing, dark room | B | Low | ✓ | ✓ | ||
Post-meal walking | 10–15 min within 30 min of meals | B | Low | ✓ | |||
Stress reduction | Daily meditation or breath-work | C | Low | ✓ | |||
CGM trial | 2–4 week wear, identify spike triggers | C | Low | * | * | * | * |
Evidence tier:
A — Well-established (multiple RCTs / meta-analyses)
B — Strong observational + supporting RCT
C — Emerging or mechanism-based
Effect size:
High — >5 mmol/mol reduction typical
Med — 2–5 mmol/mol
Low — <2 mmol/mol or indirect
* CGM is diagnostic, not therapeutic — informs choices across all four levers.
The Revi read
At Revi, we don't read your HbA1c in isolation. We look at the:
Biomarkers around it,
Biometrics that contextualise them,
Inputs you're feeding the system.
Then we identify the most likely pattern — and what to do about it.
Here's mine: The data that impacts my ability to regulate glucose & insulin.
Metric | Type | Result | Relevance |
|---|---|---|---|
HbA1c | Biomarker | Above optimal (40.77) | The marker we're investigating — drifting |
Fasting glucose | Biomarker | Optimal | No morning glucose dysregulation |
Fasting insulin | Biomarker | Optimal | Pancreas isn't over-shouting — receptors still listening |
C-peptide | Biomarker | Optimal | Pancreas working in normal range |
HOMA-IR | Biomarker | Optimal | Calculated insulin-resistance score — clean |
Adiponectin | Biomarker | Optimal | Higher = better insulin sensitivity |
ApoB | Biomarker | Above optimal (76) | Separate cardiovascular signal — independent track |
HDL | Biomarker | Below reference | Mild metabolic-pattern signal |
Triglycerides | Biomarker | Optimal (0.44) | Rules out the classic metabolic-syndrome lipid combo |
ALT / GGT | Biomarker | Optimal | Liver clean — no fatty-liver driver |
hs-CRP | Biomarker | Optimal | No systemic inflammation feeding resistance |
WHtR | Biometric | Optimal (0.479) | Below 0.5 — no visceral adiposity, rules out the biggest driver |
Sleep | Input | 6.5h (below optimal) | <7h drops insulin sensitivity ~25% the next day |
Stress | Input | High | Cortisol pushes the liver to release glucose overnight |
Alcohol | Input | 7 units/week | Disrupts overnight liver glucose regulation |
What matters most:
HbA1c above optimal, but fasting glucose, insulin, C-peptide, HOMA-IR, liver markers, hs-CRP and waist-to-height are clean.
The likely issue is not classic insulin resistance; it is probably inputs: sleep, stress, alcohol, meal timing/quality.
That makes this less of a “something is broken” pattern and more of an optimisation in advance pattern.
What I'm doing:
Starting a 2-week CGM trial — identifying which specific meals and timings spike my glucose
Extending Zone 2 cardio to 3× / week — improves insulin sensitivity for 24–48h after each session
Shifting my eating window — reducing time spent with raised glucose and insulin
Increasing dietary fibre — getting 30-40g from my diet, including 10g of Psyllium Husk
Extending my sleep window — to 7.5h with consistent timing
Adding a 10–15 minute walk after dinner — muscles use the post-meal glucose directly
Cutting alcohol to weekends only — reduces overnight glucose dysregulation
HbA1c re-tested at week 12, fasted morning draw, clean read
The principle:
That's the point of Revi — UK longevity bloodwork: not waiting until a marker is “bad”, and not reacting to one number in isolation. We look at the full pattern, then rank the levers most likely to move the result. HbA1c is one example — the full model does this across 95+ markers and the whole body.
Cris Hesketh
Founder, Revi Longevity





